Almost every new client I see living with Crohn’s disease arrives with at least one significant nutritional gap — and more often than not, several. Crohn’s disease nutrient deficiencies are not a side effect or an occasional complication. They are a predictable, almost inevitable consequence of the condition itself. Between chronic inflammation, malabsorption, restricted diets, medication interactions, and the sheer physical toll of flares, the body is constantly fighting an uphill battle to get what it needs. This is precisely why, before I look at anything else in a new consultation, I look at nutritional status first.

Why Crohn’s Disease Makes Nutrient Deficiencies Almost Inevitable
To understand why deficiencies are so common, it helps to understand what Crohn’s actually does to the digestive system. Unlike ulcerative colitis, which is confined to the colon, Crohn’s can affect any part of the gastrointestinal tract — but it most commonly targets the terminal ileum, the very section of the small intestine responsible for absorbing vitamin B12, fat-soluble vitamins, and bile salts. When that tissue is inflamed, damaged, or surgically removed, absorption of those nutrients is severely compromised regardless of how well a person eats.
Beyond the structural issue, there are several other mechanisms at play. Chronic diarrhoea accelerates transit time, meaning nutrients simply do not have sufficient contact with the intestinal wall to be absorbed properly. Reduced appetite during flares leads to lower overall intake. Many clients also self-restrict foods — cutting out dairy, raw vegetables, high-fibre foods — in an understandable attempt to manage symptoms, but this often strips the diet of key micronutrients in the process. And then there are medications: corticosteroids deplete calcium and vitamin D, methotrexate interferes with folate metabolism, and sulfasalazine blocks folate absorption too.
When a client presents with unexplained fatigue, poor wound healing, hair thinning, low mood, or frequent infections, these are not vague or psychosomatic complaints. In the context of Crohn’s disease, they are red flags for specific nutritional deficiencies that deserve urgent clinical attention.
The Most Common Deficiencies I See in Practice
After years of working with clients with inflammatory bowel disease, certain deficiencies come up time and again. Here are the ones I investigate in every single new Crohn’s consultation.
Vitamin D
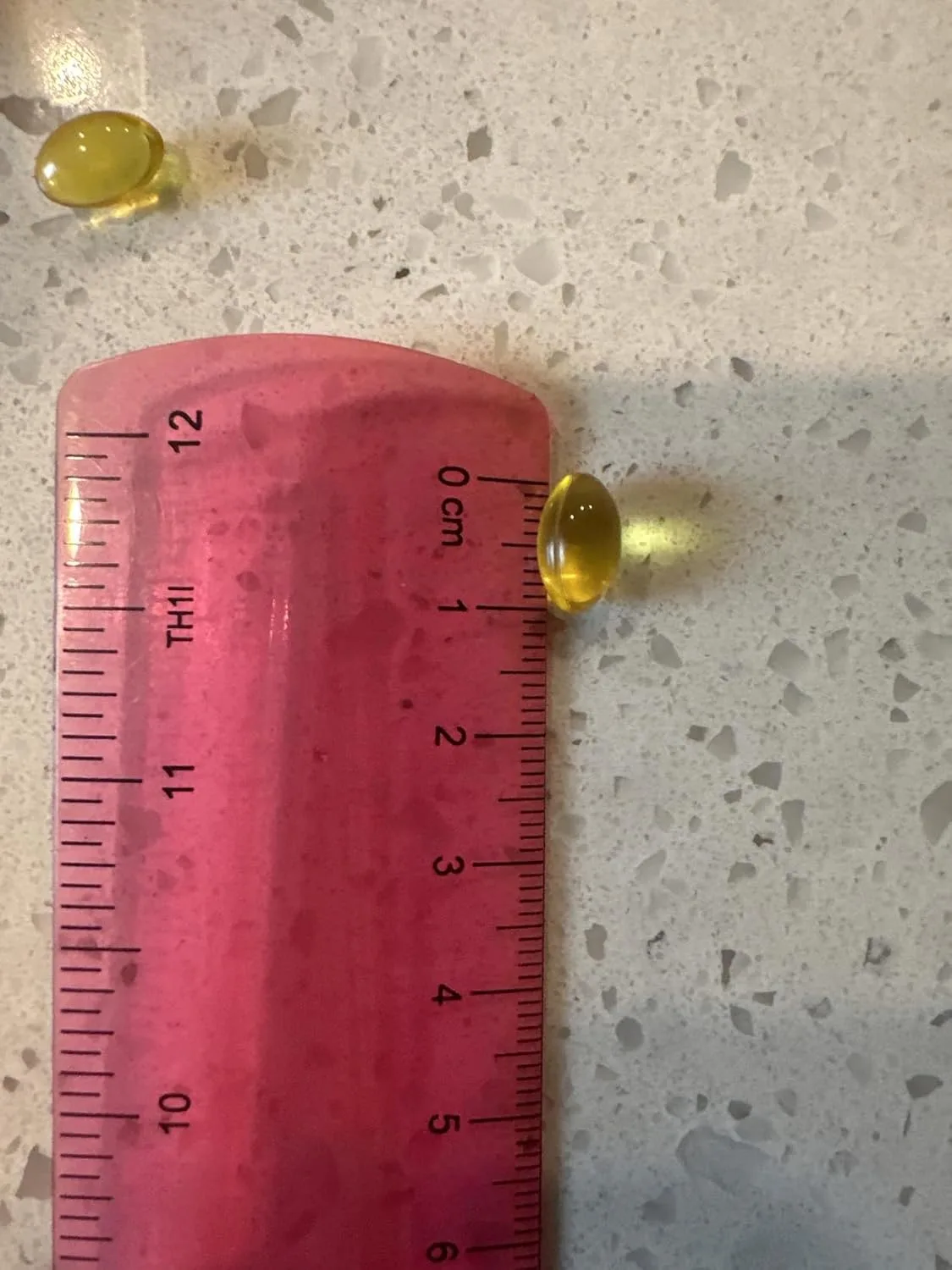
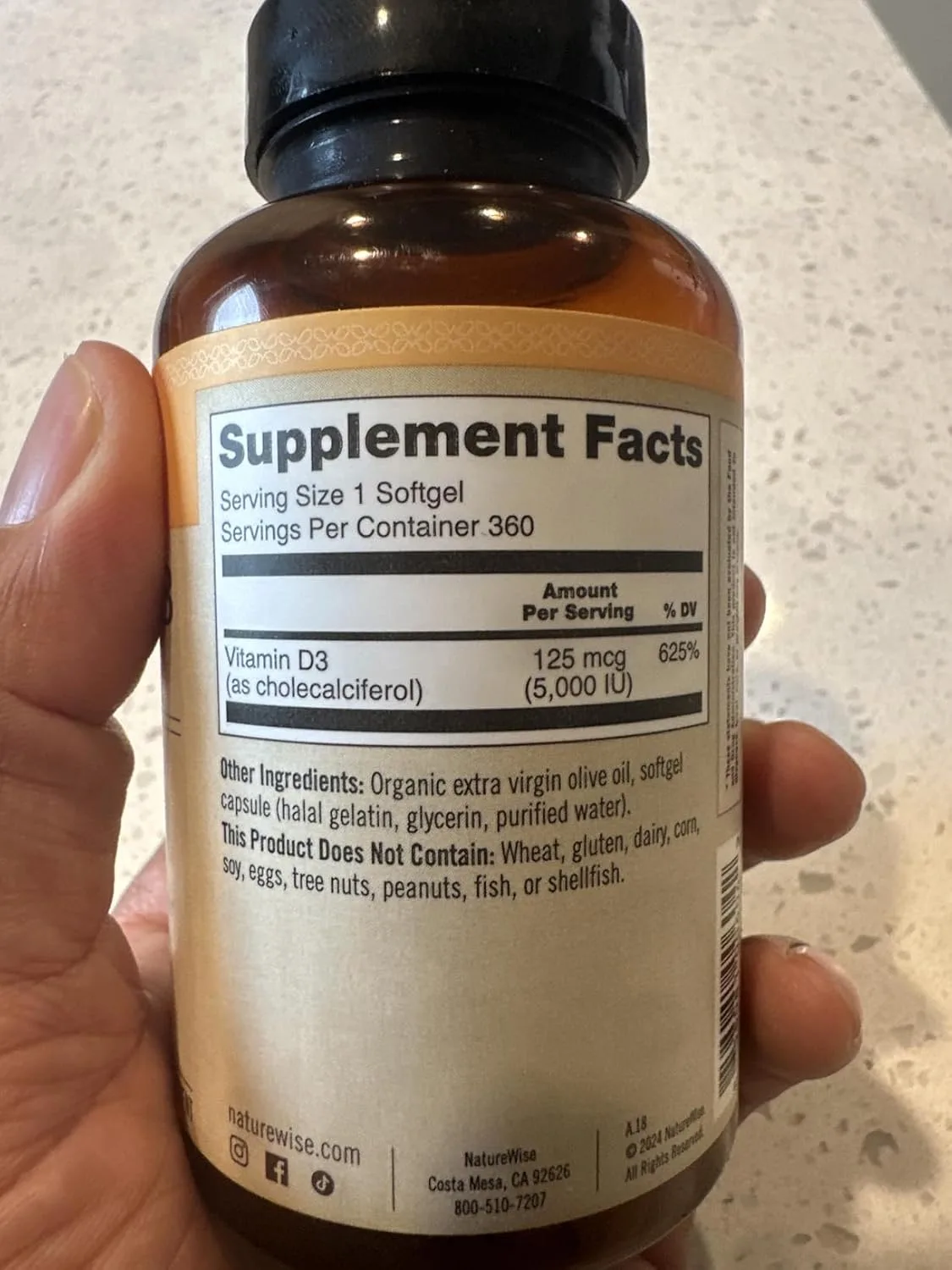
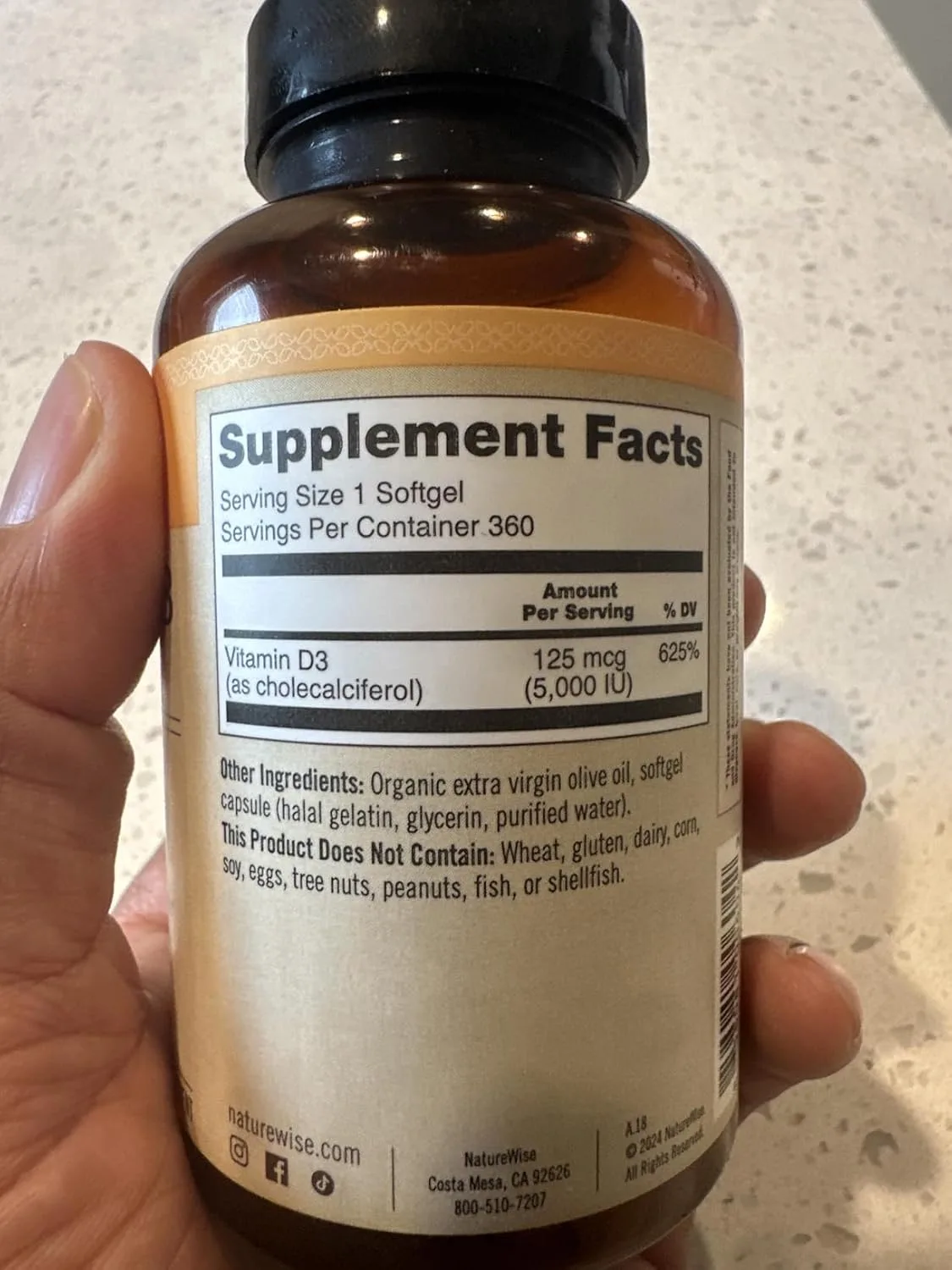
This is probably the most consistent finding in my practice. Research consistently shows that vitamin D deficiency is widespread in Crohn’s patients, and a meta-analysis of 14 studies found people with IBD had 64% higher odds of vitamin D deficiency than controls (OR 1.64), with ulcerative colitis patients at more than double the odds. Vitamin D is critical not only for bone health — already a concern in Crohn’s due to steroid use and reduced calcium absorption — but also for immune regulation. Low vitamin D has been associated with higher disease activity and increased risk of flares. I almost always recommend a quality supplement, and I often point clients toward NatureWise Vitamin D3 5000iu, a non-GMO softgel in organic olive oil that supports immune function, bone health, and healthy muscle function. For those who need a lower maintenance dose, the NatureWise Vitamin D3 2000iu version is a gentler option — both come in a one-year supply which matters for long-term management.
Iron
Anaemia is one of the most common extraintestinal complications of Crohn’s disease, and iron deficiency is a leading cause. Chronic blood loss from intestinal inflammation, poor dietary intake, and impaired absorption in the duodenum and upper small intestine all contribute. Symptoms — fatigue, breathlessness, difficulty concentrating — are often dismissed as general “Crohn’s fatigue,” which delays appropriate treatment. Ferritin levels are the most sensitive marker, and I always request them alongside a full blood count.
Vitamin B12
Because B12 is absorbed exclusively in the terminal ileum, anyone with ileal involvement or resection is at high risk. Deficiency can develop insidiously over months or years, and by the time symptoms like peripheral neuropathy or cognitive changes appear, stores are severely depleted. I recommend B12 testing every six to twelve months for clients with ileal disease, and oral or sublingual supplementation — or intramuscular injections where absorption is too compromised — is usually warranted.
Folate, Zinc, and Magnesium
These three tend to cluster together in clients who are restricting their diets significantly. Folate is depleted by methotrexate and sulfasalazine, and it is also low in diets that exclude leafy greens. Zinc is lost through chronic diarrhoea and is critical for immune function, skin integrity, and wound healing. Magnesium, often overlooked, is essential for hundreds of enzymatic processes and is commonly deficient in malabsorptive conditions — low magnesium can also worsen fatigue, muscle cramps, and anxiety, symptoms that many clients attribute solely to their Crohn’s.

Supporting Gut Health Alongside Targeted Supplementation
Correcting individual deficiencies through targeted supplementation is essential, but it works best when you are also supporting the overall environment of the gut. Chronic inflammation impairs the absorptive surface of the intestine — so even well-chosen supplements will have limited impact if the gut lining is severely compromised. This is where a broader approach to gut health becomes part of the nutritional strategy.
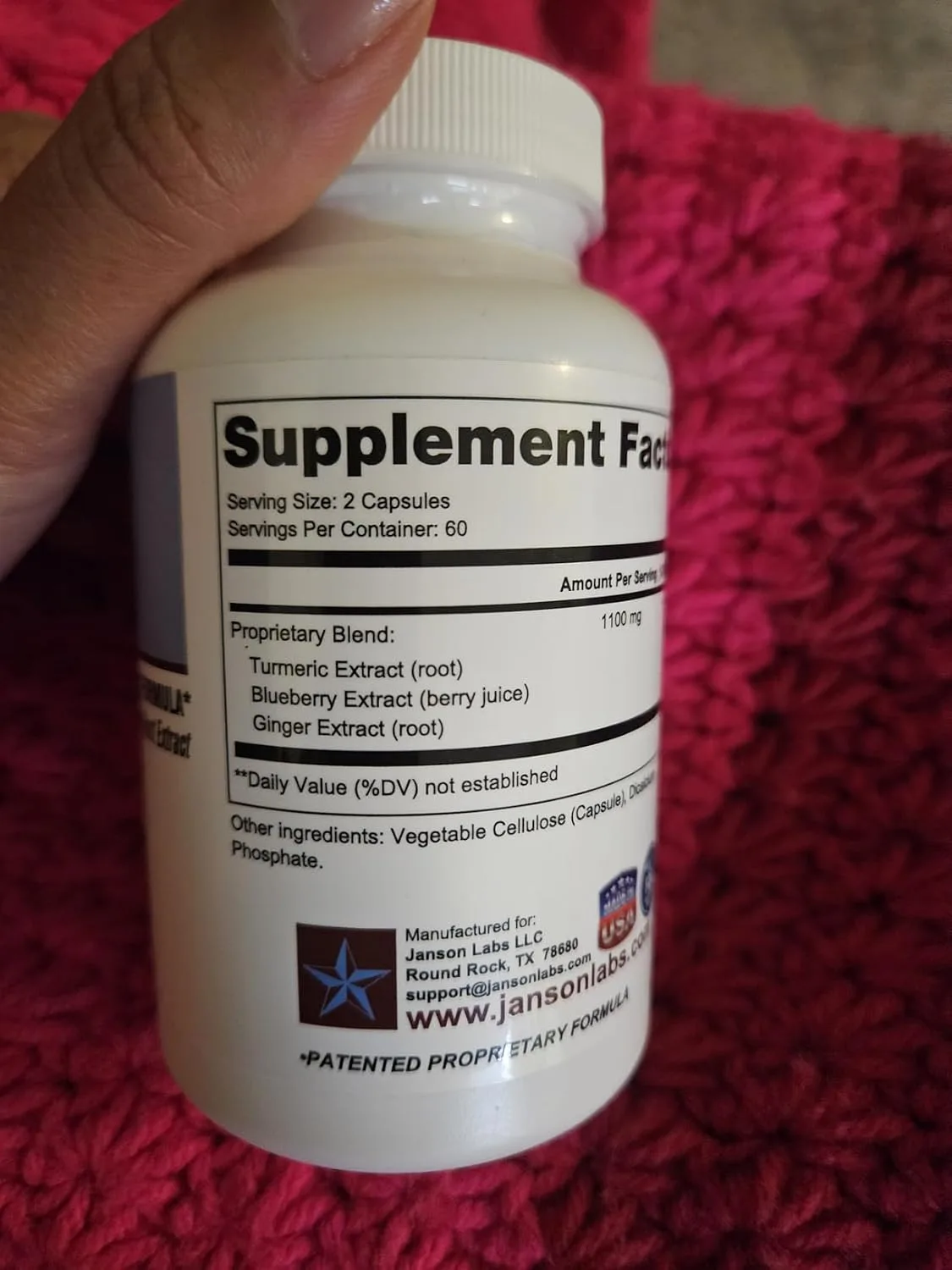
One product I have found worth discussing with appropriate clients is the JL-7 Crohn’s and Colitis Supplement, a patented, all-natural formulation designed to support gut health in the context of IBD-related GI tract inflammation including Crohn’s disease and ulcerative colitis. As always, any new supplement should be discussed with your gastroenterologist or IBD nurse, but for clients looking to take a proactive, natural approach to gut support alongside their medical treatment, this is one I consider worth exploring.
Probiotic support is another area I address carefully in Crohn’s clients. The evidence base is more nuanced here than it is for conditions like IBS, and strain selection matters. For general digestive and immune support, I sometimes recommend the Digestive Advantage Daily Probiotic Capsules, which combines digestive enzymes with probiotic support — a practical dual-action option for clients managing both digestive discomfort and nutrient breakdown. For those who specifically want an acidophilus-based probiotic to help optimise intestinal flora, the GeriCare Acidophilus with Pectin Probiotic Capsules is a cost-effective option that also supports immune defences and bone health — two areas of particular concern in Crohn’s disease.

Omega-3 Fatty Acids: An Underutilised Tool in Crohn’s Nutrition
I want to give omega-3 fatty acids their own section here because they are consistently underused by clients with Crohn’s disease despite a genuinely useful evidence base. Omega-3s — particularly EPA and DHA from marine sources — have well-documented anti-inflammatory properties. Research published in journals including Gut and Clinical Nutrition has explored their role in modulating intestinal inflammation, and while they are not a replacement for medical treatment, they represent a meaningful adjunct for many clients.
Fat malabsorption in Crohn’s also means that dietary intake of omega-3s from oily fish is often insufficient or poorly absorbed, so supplementation is frequently necessary. There are several quality options I recommend depending on a client’s needs and budget:
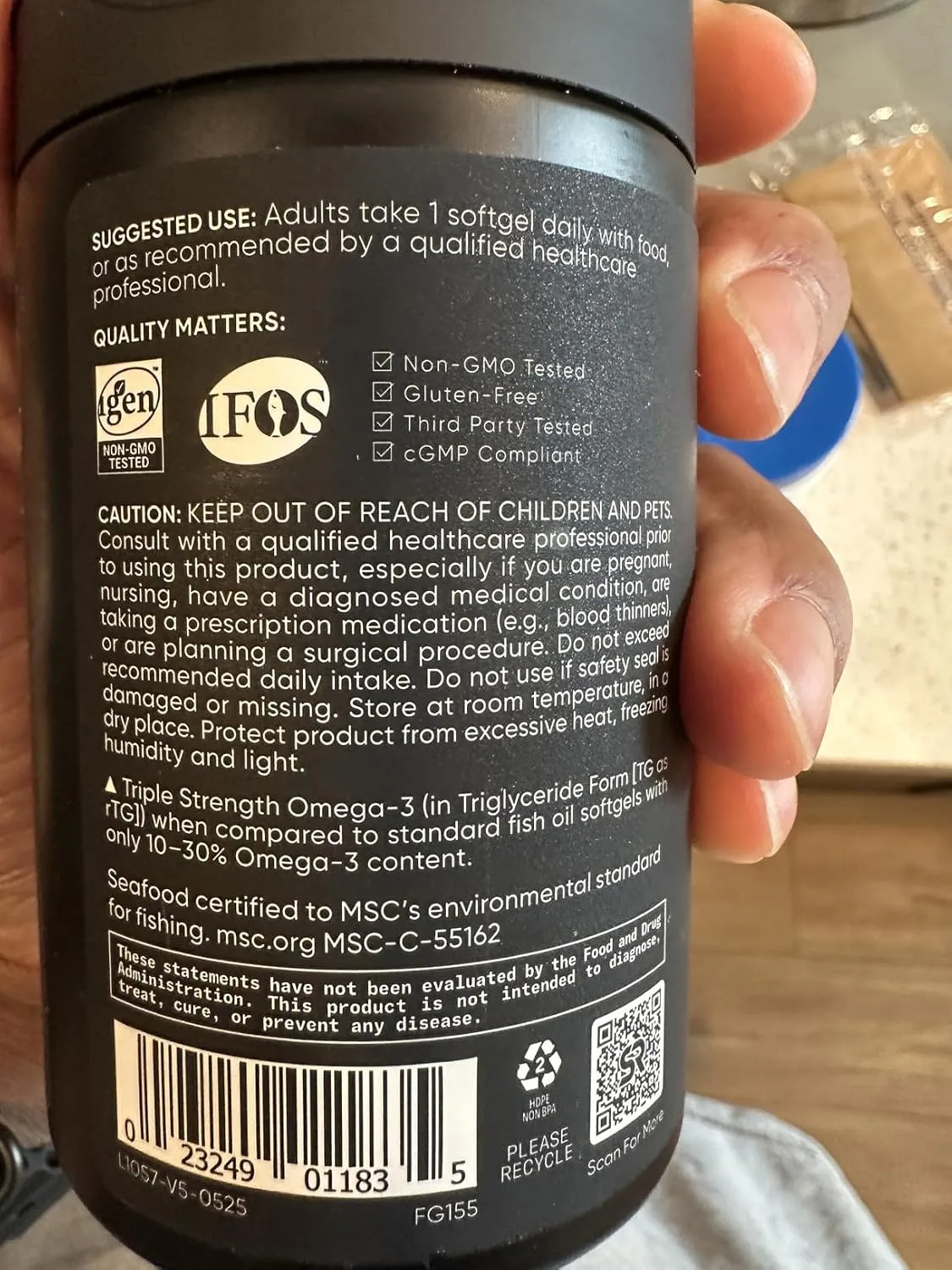
- Sports Research Omega-3 Fish Oil 1250mg — triple strength, sustainably sourced from wild Alaska Pollock, MSC certified, non-GMO and soy free. A reliable everyday option with strong sourcing credentials.
- Triple Strength DHA Omega-3 Fish Oil 3600mg — for clients who need a higher therapeutic dose, this provides over 2100mg of combined omega-3s per serving including 860mg DHA and 1300mg EPA from premium wild-caught fish. Burpless formula, which my clients particularly appreciate.
- NatureWise Extra-Strength Omega-3 Fish Oil — a well-rounded option with 600mg EPA and 400mg DHA per serving, plus vitamin E for antioxidant support and a pleasant lemon flavour. GMO-free and a good fit for clients new to fish oil supplementation.
I typically recommend omega-3 supplementation as part of a broader anti-inflammatory nutritional strategy, particularly during remission, when building nutritional reserves and reducing systemic inflammation is a primary goal.

Why Vitamin D Testing Should Come Before Supplementation in Crohn’s
Vitamin D deficiency is nearly universal in Crohn’s disease — driven by malabsorption in the small intestine, sun avoidance during flares, and sometimes medication interactions. But here’s what I’ve learned: supplementing without knowing your baseline almost always means either under-dosing or guessing.
What works
- Most clients I see with Crohn’s are sitting at 20–30 ng/mL when they test; the 5000iu dose gets measurable results within 8–12 weeks without overshooting into the toxic range for most people.
- Higher-dose D3 supplementation correlates with better bone density, fewer respiratory infections during remission, and improved mood — all documented concerns in the Crohn’s population.
- The NatureWise formulation is clean, third-party tested, and comes in an easy single-capsule dose that clients actually stick with, unlike chewables or liquids that can be irritating during flares.
What doesn’t
- If your malabsorption is severe (especially during active disease), even 5000iu may not raise your levels enough — this is why testing at baseline and again at 12 weeks is non-negotiable, not optional.
- This is not a substitute for calcium co-supplementation; vitamin D without adequate dietary calcium can paradoxically worsen bone loss, especially in clients on corticosteroids.
Vitamin D is foundational for immune regulation and bone health in Crohn’s, but it’s not a stand-alone fix — it works best as part of a broader micronutrient strategy guided by actual lab values. NatureWise Vitamin D3 5000iu is my go-to for clients with confirmed deficiency and reasonably stable absorption, but always get tested first and retest after 12 weeks.
This post contains affiliate links. As an Amazon Associate, I earn from qualifying purchases at no extra cost to you.

![Customer photo of [product description - e.g., supplement bottle/packaging]](https://digestionfaq.com/wp-content/uploads/2026/07/B01J2ZA8HI-1.webp)

![Customer photo of [product name/form - e.g., supplement bottle, capsules, powder] for Crohn's disease nutrient support](https://digestionfaq.com/wp-content/uploads/2026/07/B0DZQMPT6G-1.webp)
![Customer photo of [specific product/packaging/contents visible in image]](https://digestionfaq.com/wp-content/uploads/2026/07/B0DZQMPT6G-2.webp)


![Customer photo of [product item and what it shows]](https://digestionfaq.com/wp-content/uploads/2026/07/B01NBTJFJB-1.webp)

![Customer photo of [product description - e.g., supplement bottle, packaging, pills/capsules]](https://digestionfaq.com/wp-content/uploads/2026/07/B0C5F59RWG-2.webp)

NatureWise Vitamin D3 5000iu
I recommend this dose and formulation because clients actually take it consistently and see documented improvements in bone density and mood.
Check Price on Amazon →


